4 min read
Unique Ways to Improve Key Clinical Skills Using Aquifer
Getting students up to speed in clinic is a common challenge due to the fast pace of the clinical environment, the amount of...
Accelerated pathways leave little room for delayed integration. Structured case-based learning can help students connect molecular mechanisms to patient presentation earlier and more effectively.
Students can diagram the cytoskeleton. They can describe chloride transport. They can define lysosomal trafficking.
But when you ask, “How does this molecular defect cause this patient’s symptoms?” The explanation may turn to silence.
For faculty teaching in a BS/MD pathway, this moment may feel familiar. BS/MD students often excel at mastering foundational science content. What many still need is structured practice using that knowledge to explain what is happening in a patient.
In accelerated pathways, there is less time for those connections to develop gradually. Students are expected to move quickly from memorizing mechanisms to reasoning through patient presentations. That transition requires intentional integration between foundational science and clinical reasoning from the beginning of the curriculum.
Faculty teaching cell biology, histology, biochemistry, genetics, and related foundational science courses often face a common set of challenges:
Students can memorize pathways, but may struggle to explain clinical consequences.
Clinical examples increase engagement, but may not consistently build reasoning frameworks.
Vertical integration is a program priority, yet is hard to operationalize across courses consistently.
Faculty have limited time to build structured, clinically grounded cases from scratch.
The result is a familiar challenge: students may recall pathways accurately, but still struggle to explain how those mechanisms produce clinical findings.
Within the BS/MD accelerated track, there is less room for delayed integration. Foundational science courses need to help students connect molecular mechanisms, tissue pathology, and patient presentation as they are learning the science itself.
Many programs respond to this challenge by adding more clinical examples to foundational science courses. While examples can increase engagement, they do not always help students build durable reasoning and clinically meaningful frameworks. What students need is repeated, structured practice connecting mechanisms to patient findings.
Aquifer’s point of view is that early clinical reasoning can be built deliberately in the foundational sciences. It does not require overhauling a curriculum or turning foundational science courses into clinical courses. It requires a consistent way to anchor science in patient problems, make causality visible, and support faculty with high-quality resources that are ready to use.
One way to help students build this bridge is to begin with the patient before moving into the pathway.
Instead of presenting disease as an example after teaching a mechanism, faculty can reverse the sequence. A structured Aquifer Signature course case can introduce a patient scenario that gives students a reason to understand the underlying science. For example:
A cystic fibrosis case before membrane transport
A case with bullous pemphigoid disorder before cell adhesion
An infant hypotonia case that includes lysosomal storage disorders
Beginning with a patient problem changes how students engage with the science. The mechanism becomes an explanation for what the patient is experiencing rather than a disconnected fact to memorize.
Aquifer cases are designed to support this kind of integration. They are educator-built, peer-reviewed, clinically grounded, and structured for faculty to scale. For accelerated programs, using this approach matters in order to maintain quality while scaling. Faculty can create more meaningful integration without adding unsustainable preparation time by using thoughtfully developed cases and similar ready-to-implement teaching resources.
Students often memorize pathways without fully understanding how one mechanistic step leads to the next.
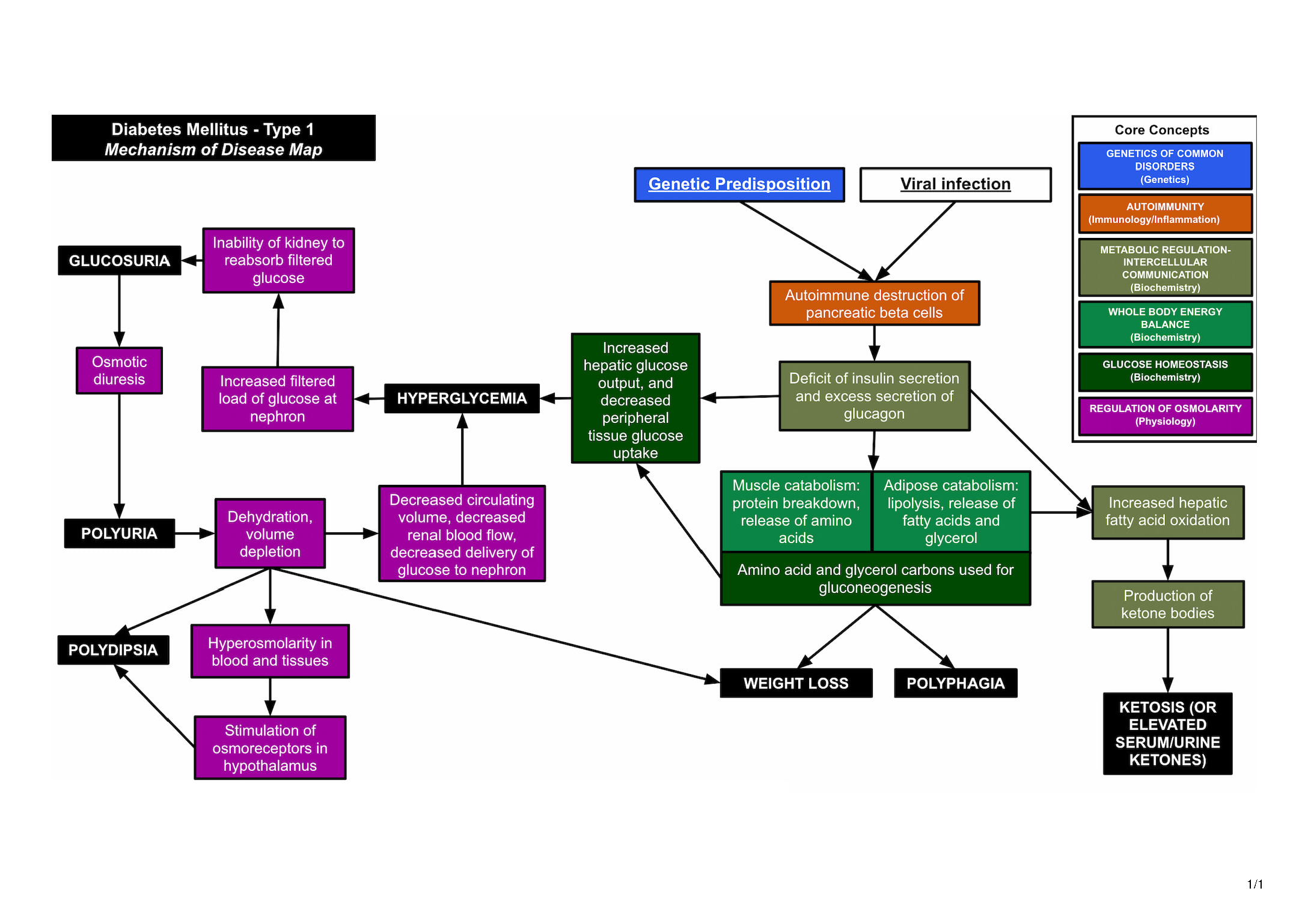
Aquifer’s Integrated Illness Scripts and included Mechanism of Disease Maps help make those relationships visible by tracing the progression from underlying disease process to clinical findings. 
Faculty can also adapt or extend an MOD map to align with course objectives. If a key mechanistic step is missing, students can be asked to identify and explain it. For example:
What step is absent between this protein defect and the tissue finding?
What cellular process explains this transition?
Where does this mechanism begin to produce the patient’s symptoms?
This type of activity reinforces deeper reasoning. Over time, repeated practice helps students recognize patterns, compare conditions, and carry foundational science forward into clinical learning.
Given limited faculty time in accelerated programs, faculty need integration strategies that are both effective and sustainable.
Assigning Aquifer Signature course cases as pre-work can create a shared baseline before class. As a result, in-class time can be intentionally focused on higher-value learning activities such as deep mechanistic exploration, comparative disease reasoning across similar presentations, and actively identifying and clarifying common misconceptions.
Faculty-created clinical integration materials can be valuable, but are difficult to sustain and scale. Thus, structured, peer-reviewed Signature Courses can help alleviate this burden by providing high-quality, ready-to-use materials that maintain academic rigor while reducing the need for extensive content creation. At the same time, they promote consistency across sections and campuses, which is especially important for programs aiming to achieve strong vertical alignment within their curricula.
This approach helps preserve class and faculty time for the work that most benefits students: faculty guided reasoning, discussion, clarification, and application.
BS/MD programs continue to expand, while expectations for student readiness remain high.
If foundational courses do not intentionally cultivate mechanistic clinical reasoning, the burden shifts downstream. Clinical reasoning does not need to wait until M1; it may begin when mechanisms are first introduced. When students connect:
Molecular defect → Cellular consequence → Tissue pathology → Patient presentation
They stop memorizing and start thinking like physicians. The connections between core concepts and the key presenting features of common clinical conditions improve learner understanding of the “why” behind their occurrence and, as a consequence, increase the cognitive connection needed for long-term recall and the deeper understanding needed for higher-quality clinical practice.
If your institution already subscribes to Aquifer, this may be the right time to revisit how your resources are being used in foundational science courses.
Consider:
Are foundational science faculty leveraging Aquifer Signature Courses as anchors for clinical integration?
Are Integrated Illness Scripts being used systematically to support mechanistic reasoning?
Are cases assigned as supplemental material, or are they intentionally connected to course objectives and in-class activities?
A Curricular Consult can help your program identify where Aquifer Signature courses, Integrated Illness Scripts, and Mechanism of Disease Maps may fit into or enhance your foundational science curriculum.
If your BS/MD pathway is grappling with how to strengthen early clinical reasoning without overhauling the curriculum, structured case-based integration may be the most efficient starting point.
The goal is not to add more content. The goal is to help students use foundational science more effectively when they begin to encounter real clinical settings.
Aquifer can help programs build that bridge with tools that support the connection between mechanisms of disease and patient presentation. Request a demo to learn more.

4 min read
Getting students up to speed in clinic is a common challenge due to the fast pace of the clinical environment, the amount of...

6 min read
“There is only one way to eat an elephant: a bite at a time.” (Desmond Tutu) Making a small change in the way you teach can have a...

4 min read
Aquifer Integrated Illness Scripts are new teaching and learning tools designed to link basic science and clinical knowledge and drive...